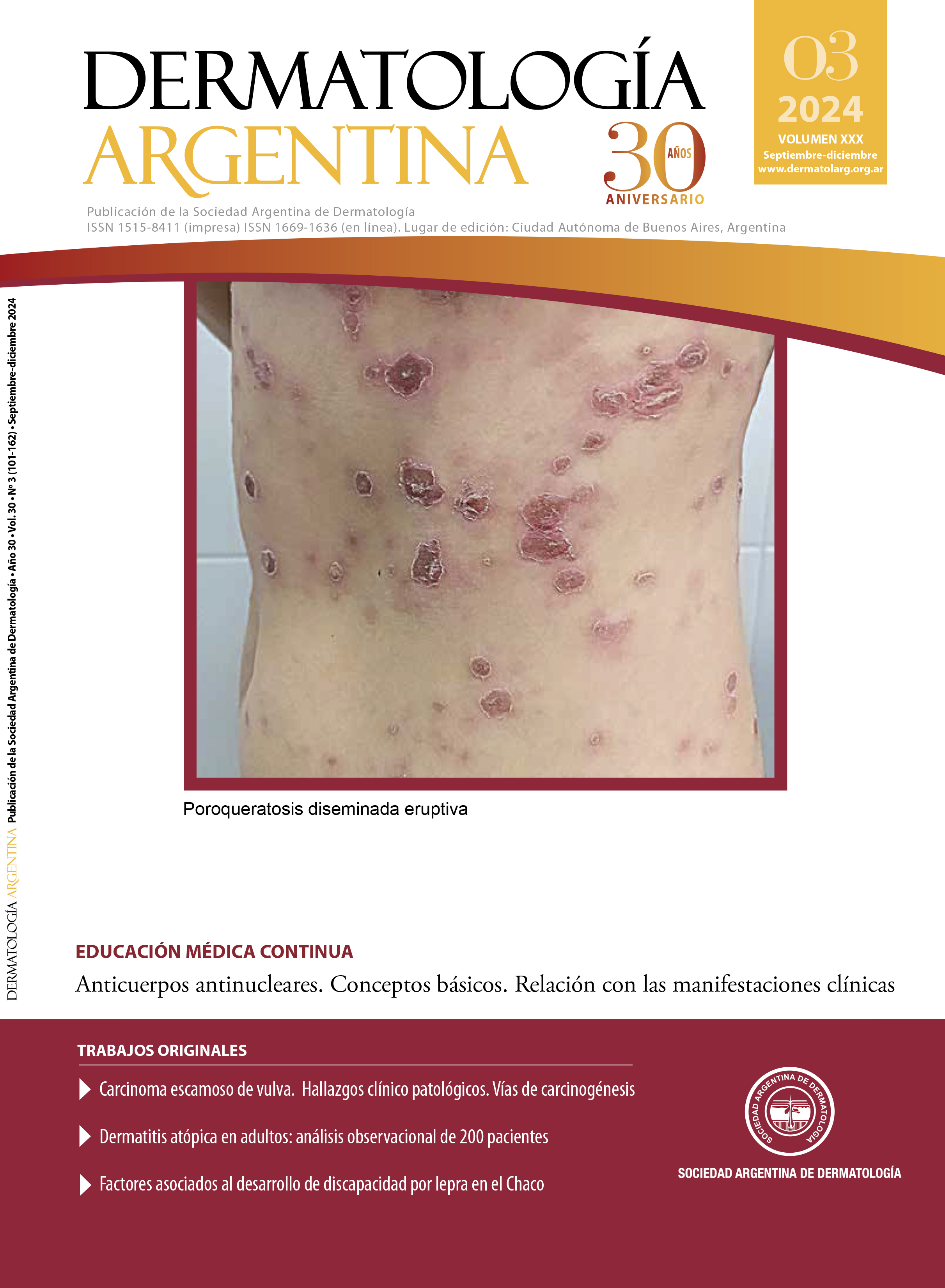
Eruptive disseminated porokeratosis
DOI:
https://doi.org/10.47196/da.v30i3.2672Keywords:
porokeratosis, cornoid lamellaAbstract
Porokeratosis is a heterogeneous and rare group of acquired or inherited dermatoses of unknown etiology, characterized by a keratinization disorder secondary to an abnormal clonal expansion of keratinocytes. Eruptive disseminated porokeratosis (EDP) is an atypical variant with abrupt onset with more than 100 lesions involving multiple regions. It is subdivided into paraneoplastic, inflammatory, idiopathic and associated with immunosuppression. The case of a 28-year-old woman who consulted is presented. due to pruritic erythematous annular plaques with atrophic center and hyperkeratotic border of generalized distribution, with compatible dermoscopy and histopathology and partial response to topical treatment.
References
I. Gimeno Castillo J, De la Torre Gomar FJ. FR- Formulación tópica de estatinas y colesterol como tratamiento de poroqueratosis. Actas Dermosifiliogr. 2023;114:533-535.
II. Bonilla JD, Alzate B K, Motta A. Pápulas con bordes hiperqueratósicos en áreas fotoexpuestas. ¿Qué aporta la dermatoscopia? Rev Asoc Colomb Dermatol Cir Dermatol. 2021;29:229-232.
III. Yalcin B, Uysal PI, Kadan E, Bozdoğan Ö. Eruptive disseminated porokeratosis in a patient with type 2 diabetes mellitus. Am J Dermatopathol. 2016;38:125-127.
IV. Mangas C, Espeli V, Blum R. Un caso de poroqueratosis diseminada eruptiva en un paciente oncológico tratado con trastuzumab y exemestano: ¿fenómeno asociado al cáncer o inducido por fármacos? Actas Dermosifiliogr. 2018;109:559-560.
V. Shoimer I, Robertson LH, Storwick G, Haber RM. Eruptive disseminated porokeratosis: a new classification system. J Am Acad Dermatol. 2014;1:398-400.
VI. Pedrozo L, Rodríguez Saa S, Cohen-Sabban EN, Cabo H. Dermatoscopia de la poroqueratosis actínica superficial diseminada. Dermatol Argent. 2015;21:76-77.
VII. Valiente-Rebull C, Rodríguez L, Martínez-Braga G, Di Martino-Ortiz B, et ál. Poroqueratosis. Informe de tres casos. Our Dermatol Online. 2014;5:163-168.
VIII. Montes-Torres A, Camarero-Mulas C, De Argila D, Gordillo C, et ál. Poroqueratosis pruriginosa diseminada inflamatoria. Buena respuesta a ciclosporina. Actas Dermosifiliogr. 2016;107:261-262.
IX. Cazorla MB, Müller G, Yarza M, Navacchia D, et ál. Poroqueratosis de Mibelli en la edad pediátrica. Dermatol Argent. 2020;26:32-34.
X. Vargas-Mora P, Morgado-Carrasco D, Fustà-Novell X. Poroqueratosis. Revisión de su etiopatogenia, manifestaciones clínicas, diagnóstico y tratamiento. Actas Dermosifiliogr. 2020;111:545-560.
Downloads
Published
Issue
Section
License
Copyright (c) 2024 on behalf of the authors. Reproduction rights: Argentine Society of Dermatology

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
El/los autor/es tranfieren todos los derechos de autor del manuscrito arriba mencionado a Dermatología Argentina en el caso de que el trabajo sea publicado. El/los autor/es declaran que el artículo es original, que no infringe ningún derecho de propiedad intelectual u otros derechos de terceros, que no se encuentra bajo consideración de otra revista y que no ha sido previamente publicado.
Le solicitamos haga click aquí para imprimir, firmar y enviar por correo postal la transferencia de los derechos de autor